

This blog-post is intended to provide the information required for the ALS practitioner to complete their theory component for the 2018 CPG update with regard to TXA. To access CPD points for this activity (blog post) please see the information box at the bottom.
This resource may also be used to inform any interested party in the physiology, pharmacology and use of Tranexamic Acid in the emergency setting.
Some definitions before we start

First of all – Let talk about clotting
The coagulation cascade is something we need to have a basic understanding of if we are to understand where TXA works, and how it works.
The focus of the information presented here will be around the trauma patient, but the information presented can be extrapolated to any patient with major bleeding, and activation of the clotting and fibrinolysis cascade.
The first thing we need to understand, is that where there is bleeding (as a result of trauma, or damage to vessels, vessel rupture), there is clotting. Where there is clotting, there is an internal process of fibrinolysis (break down of clots). The body is continuously aiming to achieve an environment that is in homeostasis, or balance. When a clot is formed, it puts distal tissue at risk, and so it must be broken down eventually.
This is completely normal. Refer to diagram below and description that follows to understand the coagulation cascade a little better:

http://derangedphysiology.com/files/Coagulation%20cascade.pdf
1: Resting Platelets
- Platelets can be thought of as sentries floating around the body, alerting the system if there is a problem noted.
- Healthy cells in the vasculature produce the following chemicals which inhibit platelet aggregation
- Nitrous Oxide (vasodilator)
- Prostcyclin
- Damaged cells make less of the chemicals above and so there is increased chance of clotting in vessels
- Healthy cells in the vasculature produce the following chemicals which inhibit platelet aggregation
- Platelets have receptors on them, that if activated, will increase the risk of clotting and platelet aggregation
- ,These receptors are activated by the following:
- Thrombin, thromboxanes and collagen (these are usually present when there has been some trauma to the endothelial lining of the vessel)
- ,These receptors are activated by the following:
2: Platelet Adhesion
- When receptors are activated on the platelet, there are a whole lot of changes that occur
- The receptors on the platelets are activated by collagen exposure to the blood (it should be covered by the protective lining of endothelium)
- Platelets cover the collagen and release a whole load of chemical mediators
3: Platelet Activation
- Once the chemicals are released from platelets that have already stuck to collagen
- Chemicals include:
- ADP, thromboxane A2, serotonin, platelet activation factor and thrombin
- The more platelets are added to the clot, the more the platelets release the chemicals above and the more platelets are added to the clot
- Chemicals include:
Below is an image of the triggers to platelets, and the effects when the platelet receptors are activated.
4: Platelet Aggregation
- Mediators and Calcium are released, resulting in more platelets joining the clot, this activates more platelets, and results in the positive feedback mechanism that is the clotting cascade.
5: Clot formation
- Local stimulation of the clotting factors occurs and tissue factors are released.
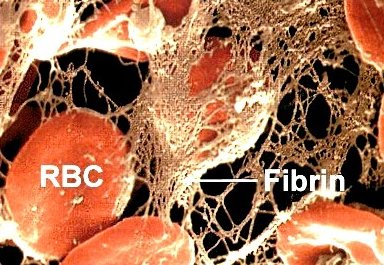
- Thrombin joins the clot resulting in the conversion of fibrinogen to fibrin, this strengthens the clot
- Fibrin is a tough fibrous material that bulks up the clot and weaves the red blood cells and platelets together more tightly to hold the clot together
 http://www.daviddarling.info/encyclopedia/F/fibrin.html
http://www.daviddarling.info/encyclopedia/F/fibrin.html
6: Clot Fibrinolysis
All clots will need to be broken down again with time, as soon as there is local activation of the clotting factor, there is also local fibrinolysis. This is a safety mechanism to prevent damage to the tissues distal to the injury in the vessel, and assists with healing.
This is helpful with small injuries to the vessels, however, in patients who have a systemic activation of clotting due to massive or severe trauma, the activation of systemic fibrinolysis can increase the threat to life.
Where there is massive clotting, there is massive fibrinolysis, and this is counter productive in the patient who is bleeding to death.

Plasmin
Plasmin is an enzyme that destroys the fibrin mesh, this breaks down the clot into smaller fragments which are then circulated through the body and broken down further in other areas of the body (the liver and the kidneys).
The problem is that when this happens on a mass scale, there is a problem in that clotting and then bleeding on a mass scale also occur resulting in consumption of the coagulation factors, and with increased bleeding, this means the patient cannot clot and maintain a clot. This is further discussed below.
The Life threatening bleed
This brings us to the patient who presents with a life threatening bleed.
See the diagram below for the processes that can result in traumatic coagulopathy:

https://ccforum.biomedcentral.com/articles/10.1186/cc12685
Trauma results in tissue damage, which results in three negative effects
- Cytokine and inflammatory mediator release
- Blood loss through the damage to the vessels
- Activation of clotting (and by default, fibrinolysis)
What is really important to understand, is that tranexamic acid alone will NOT save the patient with major haemorrhage, a multi-pronged approach to the management of this patient is vital. This approach should include:
- Control where possible of bleeding with pressure, tourniquets, and splinting as needed
- Limited, or careful fluid administration to the patient with a major bleed
- Limiting crystaloid volume as far as possible
- Starting blood products and/or inotropes earlier rather than later to maintain perfusion to keep the patient alive
- Early and rapid transportation to a facility capable of coping with the patient’s condition
If the patient has possible raised intracranial pressure, the recipe above is slightly different and will be discussed under the guideline update for the patient with raised intracranial pressure.
What we do know, is that in the patient with massive blood loss, when we add tranexamic acid to the care bundle above, early in the patient treatment (the earlier the better), we can affect mortality positively.
What are the recommendations?
- Tranexamic acid is recommended for administration AS EARLY AS POSSIBLE to the trauma patient who is bleeding or at risk of significant bleeding.
-
At a loading dose of 1g over 10 minutes for adult patients, followed by an infusion of 1g over 8 hours (HPCSA PBEC CPG, 2018)
-
- IV Tranexamic acid should be used as soon as possible in patients with major trauma or active, or suspected active bleeding (HPCSA PBEC CPG, 2018)
- Tranexamic acid should not be used if the time since injury is more than 3 hours (except in special circumstances, such as evidence of hyperfibrinolysis exists)
- Protocols for the administration of Tranexamic acid should allow for the administration of this mediaction on route to hospital.
What is the effect of this medication on mortality?
The Crash-2 trial (Shakur, et al. 2010) enrolled over 20 000 patients who were admitted with bleeding or thought to be at risk of bleeding, these patients were randomized to one of two groups.
The first group received 1g TXA over 10 minutes followed by a 1g infusion over 8 hours. The second group received placebo at the same time regime as the TXA group (the treating practitioners were not aware if the patient received the medication or placebo). This was administered in the first 8 hours following injury.
The Crash-2 trial (Shakur, et al. 2010) reported the following findings:
- Primary outcome:
- Mortality at 4 weeks post admission was decreased in the group who received TXA for all patients
- Risk of death due to bleeding was also reduced in the TXA group.
- No increased risk of thrombo-embolic events (this means that there was no increase in the risk of clotting in the patients in this study)
- Subgroup analysis (secondary outcome)
- Patients who received the medication within 1 hour of thier injury, then the risk due to death from bleeding was reduced even further.
- TXA given at 1-3 hours following injury still had an imporvement in mortality.
- TXA given after 3 hours did not improve mortality, but actually was associated with increased the risk of death.
Description of the medication:

- Tranexamic acid (trade name: Cyklocapron)
- Classed as: Anitfibrinolytic agent (refer above for more info)
- Schedule: 4 (please refer to the “understanding scheduling” section for more information)
Pharmacological Action (how does the medication work?)
Tranexamic is a medication that prevents the breakdown of clots (antifibrinolytic), the important thing here is that tranexamic acid DOES NOT create clots, that process happens as it normally would, TXA only prevents the breakdown of existing clots.
How does it do this?
TXA works to inhibit the activation of plasminogen to plasmin, on the diagram below you will see that in order for the clot to be broken down plasminogen (inactive form) needs to be converted to plasmin, and then the process of clot fibrinolysis can occur.
TXA is a competitive inhibitor (it works against) plasminogen activator, and so prevents plasmin from being formed.
Pharmacokinetics (how the medication moves into and out of the body)
TXA is administered to the bleeding trauma patient via IV, this means that all of the dose is immediatly available in the blood after administration.
- TXA travels in the blood almost completely bound to plasminogen
- Less than 5 % of the medication is metabolised, and so there are no by-products or metabolites of the medication after administration
- The medication is eliminated from the body via the kidneys with more than 90% of the drug excreted within 24 hours in most patients (Drugbank. 2018)
- Duration of action is approximatly 3 hours (this is why the infusion is started to maintain the antifibrinolytic effects until bleeding can be controlled) (Sukeik, 2011)
Indications (when should I use it)
When you are treating a bleeding patient, or a patient who you think might be bleeding enough to create a life threat, within the first 3 hours following injury.
- Hypotensive trauma patient with signifigant mechanism of injury and/or ongoing bleeding (HPCSA PBEC CPG. 2018)
- Within the first three hours following injury
Contra-Indications (when should I NOT use it)
The list in red is the list of contrindications that appear on the package insert of this medciation. The list that appears in blue below that is a list of relative contraindaitons, and conditions in which the provider should think a little more carefully about the risk/benefit ratio.
- In patients with acquired defective color vision, since this prohibits measuring one endpoint that should be followed as a measure of toxicity
- In patients with subarachnoid hemorrhage. Anecdotal experience indicates that cerebral edema and cerebral infarction may be caused by CYKLOKAPRON in such patients
- In patients with active intravascular clotting (for example disseminated intravascualr coagulation)
- In patients with hypersensitivity to tranexamic acid or any of the ingredients
- Known history of severe renal failure
- Liver impairment (SAMF, 2014)
- Massive upper renal tract bleed (this is not particularly relevent for the trauma environment as the patient will be bleeding from the trauma and not a renal system issue, but may be relevent in the medical patient) (SAMF, 2014)
Relative Contra-indications/precautions
- Do not delay more urgent critical resuscitation interventions to give TXA (like stopping bleeding, oxygenation, ventilation or any other life saving intervention)
- Be careful in patients at risk of thrombotic complications, e.g. procoagulant disorders, previous DVT / PE
- Renal failure patients in general
Adverse effects (things that could go wrong if I use it)
Ones we need to worry about for the pre-hospital environment
- Hypotension when intravenous administration exceeded 1 ml per minute or 100mg/min have been reported (Xanodyne Pharmaceuticals Inc)
- Anaphalaxis is a possible but rare side effect of TXA (6 cases reported)
Other adverse effects
- Gastrointestinal disturbances (nausea, vomiting, cramps)
- Only found with oral administration of the medication
- Seizure risk seems to increase
- Specifically in patients undergoing cardiovascular surgery, especially when the medication is administered into the spine/around the spinal nerves (epidural/spinal)
- Increased risk of thrombo-embolism
- Pulmonary Embolism, DVT and AMI: seems to be related to higher doses (reported in 4 patients who all received high doses (3-24g) daily for a prolonged period of time) (Calapai, et al. 2015), or were medical patients who presented with other risk factors present for thromboembolic disease at the time.
- Myopathy (structural or functional impairment of muscle fibres) with prolonged or chronic use of the medication (also very rare)
Severe adverse reactions to TXA are uncommon, especially in the population of patients treated in the pre-hospital environment. The risks associated with lower doses (as
reccomended below) as acute/single doses increase the safety of this medication.

Packaging
- Clear, colourless solution
- 500mg/5ml (100mg/ml solution)

Dosing
- Loading dose of 1g/10minutes followed by a 1g over 8 hour infusion
Dosing for paediatric patients
|
Age |
Loading dose (administer within 3 hours) |
Subsequent dose |
|---|---|---|
|
≥12 years::adult protocol |
1 g intravenously over 10 minutes |
1 g intravenous infusion over 8 hours |
|
<12 years |
15 mg/kg intravenously over 10 minutes (maximum dose 1 g) |
2 mg/kg/hr intravenous infusion over 8 hours or until bleeding stops |
TO ACCESS CPD POINTS FOR THIS ACTIVITY (SA only):
please email training@aiem.co.za
References:
- Calapai G, Gangemi S, Mannucci C, Miniullo PL, Casciaro M, et al. 2015. Systematic Review of Tranexamic Acid Adverse Reactions . J Pharmacovigilance 3:171. doi:10.4172/2329-6887.1000171
- Drugbank. 2018. Tranexamic Acid. available online: https://www.drugbank.ca/drugs/DB00302. Accessed 06/09/2018
- Royal College of Paeditrics and Child Health Care. 2012. Evidence Statement
Major trauma and the use of tranexamic acid in children. Available Onlne: https://www.rcem.ac.uk/docs/External%20Guidance/10k.%20Major%20trauma%20and%20the%20use%20of%20tranexamic%20acid%20in%20children%20Evidence%20statement%20(RCPCH,%20Nov%202012).pdf [accessed 06/09/2018]
- Shakur H, Roberts I, Bautista R, Caballero J, Coats T, Dewan Y, El-Sayed H, Gogichaishvili T, Gupta S, Herrera J, Hunt B, Iribhogbe P, Izurieta M, Khamis H, Komolafe E, Marrero MA, Mejía-Mantilla J, Miranda J, Morales C, Olaomi O, Olldashi F, Perel P, Peto R, Ramana PV, Ravi RR, Yutthakasemsunt S. 2010. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant hemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010, 376: 23-32.
- SAMF. 2014. South African Medicines Formulary. Division of Clinical Pharmacology, Faculty of Health Sciences, UCT. Health and Medical Publishing Group of SA.
- Sukeik M, Alshryda S, Haddad FS, Mason JM. 2011. Systematic review and meta-analysis of the use of tranexamic acid in total hip replacement. Journal of Bone and Joint Surgery
Series B. 2011;93 B(1):39-46.
- “Product Information. LYSTEDA (tranexamic acid).” Xanodyne Pharmaceuticals Inc, Newport, KY
Post by @epicEMC

Leave a comment